
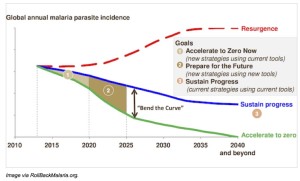
 About ten years ago, the global health community was cautious about aiming at malaria eradication. The experiences from the 1960s and 1970s left some severe scars on such campaigns. Recently, the Gates Foundation has led the shift in approach and mobilised others to join efforts to end the disease. However, while malaria is preventable and treatable, eradication requires new tools (see figure).
About ten years ago, the global health community was cautious about aiming at malaria eradication. The experiences from the 1960s and 1970s left some severe scars on such campaigns. Recently, the Gates Foundation has led the shift in approach and mobilised others to join efforts to end the disease. However, while malaria is preventable and treatable, eradication requires new tools (see figure).
A good vaccine would be highest on the agenda. Although vaccine trials show promising results, the vaccine efficacy is unfortunately too low to eradicate the disease.
Our recent study on the prevention of malaria in the Rift Valley of Ethiopia also shows some of the limited effects of insecticide-treated bed nets. In addition, we have observed that many of the mosquito bites take place at times when people do not use their bed nets. Our mosquito studies show that indoor residual spraying with insecticides can reduce the density of mosquitoes both inside the houses as well as outside the houses. Furthermore, a recent and unpublished study from south-west Ethiopia supporter previous findings that improving housing can reduce the entomological inoculation rates, which is a measure on how dangerous the mosquitoes are in transmitting malaria.
We, therefore, also support that several new tools are required. So, maybe the time is right to assess the combination of many interventions that would include active case finding, treatment, insecticide treated bed nets, indoor residual spraying, improved housing, and other vector control measures; such as reducing the out-door density of malaria mosquitoes.
 Dr. Donald A. Henderson, who led the World Health Organization’s war on smallpox, administering a smallpox vaccination in Ethiopia, around 1972. The last known case was in 1977. (Photo WHO)
Dr. Donald A. Henderson, who led the World Health Organization’s war on smallpox, administering a smallpox vaccination in Ethiopia, around 1972. The last known case was in 1977. (Photo WHO)