
The aim of the RMM (Reducing Maternal Mortality) programme in Saggen, Gamo Gofa Zone and in Basketto is to reduce maternal and neonatal deaths.
 During the first phase (2008 – 2011), we worked to set up and strengthen institutions doing Comprehensive Emergency Obstetric care (CEmOC). Arba Minch Hospital was the training centre, Saula Hospital and Chencha Hospital, and Kemba, Basketto and Melo Health Centres started to do caesarean sections through support by our project. All these institutions are now regularly doing caesarean.
During the first phase (2008 – 2011), we worked to set up and strengthen institutions doing Comprehensive Emergency Obstetric care (CEmOC). Arba Minch Hospital was the training centre, Saula Hospital and Chencha Hospital, and Kemba, Basketto and Melo Health Centres started to do caesarean sections through support by our project. All these institutions are now regularly doing caesarean.
The challenge we noted during the first phase was that large populations living in our target areas still have limited access to delivery services.
During the second phase (2012 – 2016) we aim to increase the coverage of Basic and Comprehensive Emergency Obstetric Care. Our aim is to improve the access to delivery services. We do this by strengthening health centres to do Basic Emergency Obstetric Care. We also link the work at these health centres to health posts in the kebeles, and to improve referrals to institutions doing caesarean sections.
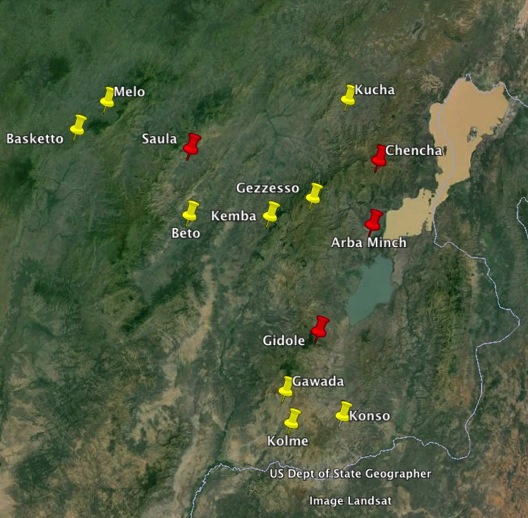
During the last year the number of institutions doing Comprehensive Emergency Obstetric care (CEmOC) has increased by four; in Bonke woreda (Gezzeso), in Beto and in Selam Berr (Kucha), and in Kolme and in Gawada.. The map shows the institutions doing CEmOC on the area. So, The number of institutions doing comprehensive emergency care is now about one institution per 250.000 people, a great improvement since 2007 when the figure was one institution per 2.5 million people.
We also collaborate with the Midwife School in Arba Minch, and currently they are evaluating how well the midwives that graduated from their school are performing (See Master thesis by Rahel Tesfaye). This will give us essential information on how to improve the quality of midwife training, and thus of RMM work.
To monitor this work and see if the project meets its societal objectives (reduced death rates), we register births and maternal deaths in four woredas with a population of about 600.000. In a recent research we have shown that it is possible to achieve high coverage community birth registration in rural Ethiopia. Such registration can be an important tool to monitor births and birth outcomes such as maternal mortality in resource-limited settings (Yaliso et al 2014, PLoSONE in press). Our results (unpublished) show that maternal deaths have since 2008 been reduced by 2/3. The institutional delivery rates have also increased substantially, and the use of traditional birth attendants is decreasing. We also see some early signs of decreasing neonatal deaths. In some areas the institutional delivery rates approach 60%.
Even if our results are encouraging, many challenges remain. The birth registration shows that highest maternal deaths rates are among women who live in remote areas, and among women who report illness during pregnancy. One study show that children born to poor women have higher death rates compared with richer families. So, in the coming years will focus on improved quality of care, particularly focusing on improving access, and on managing illness during pregnancy. We will also try to develop tools to identify the poor that are in need of special attention.
Publications
Yaya Y, Data T, and Lindtjørn B. Maternal mortality in rural south Ethiopia: Feasibility of community-based birth registration by Health Extension Workers. (Manuscript submitted 2014).
Yaya Y, Eide KT, Norheim OF, Lindtjørn B (2014) Maternal and Neonatal Mortality in South-West Ethiopia: Estimates and Socio-Economic Inequality.PLoS ONE 9(4): e96294. doi:10.1371/journal.pone.0096294
Girma M, Yaya Y, Gebrehanna E, Berhane Y, Lindtjørn B. (2013). Lifesaving emergency obstetric services are inadequate in south-west Ethiopia: a formidable challenge to reducing maternal mortality in Ethiopia. BMC Health Services Research 2013; 13(1):459.
Yaya Y, Lindtjørn B (2012). High maternal mortality in rural south-west Ethiopia: estimate by using the sisterhood method. BMC Pregnancy and Childbirth 2012; 12: 136.
Rahel Tesfaye. Client Satisfaction with Delivery Care Services and Associated Factors in the Public Health Facility of Gamo Gofa Zone, South West Ethiopia. 2014. Arba Minch University and Addis Continental Institute of Public Health.
For complete list of publications from this project click here.

 There are unfortunately many hospitals in Ethiopia and in Africa that do not work as expected. They lack staff, or equipment. Often they lack staff doing essential interventions such as caesarean sections.
There are unfortunately many hospitals in Ethiopia and in Africa that do not work as expected. They lack staff, or equipment. Often they lack staff doing essential interventions such as caesarean sections.