
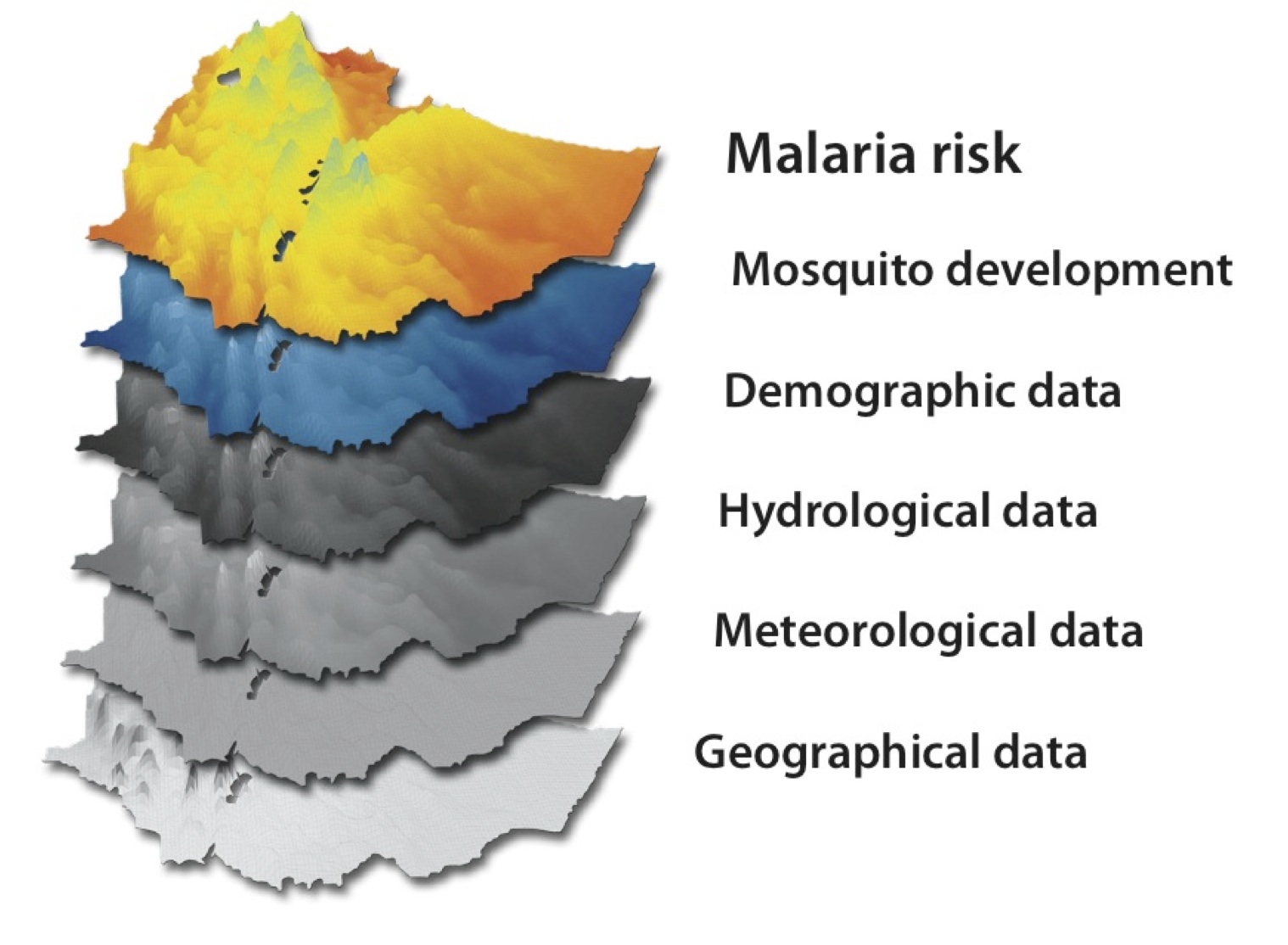
 The Ethiopian Malaria Prediction System (EMaPS) combines information about weather and water with demographic data to predict mosquito development and malaria risk.
The Ethiopian Malaria Prediction System (EMaPS) combines information about weather and water with demographic data to predict mosquito development and malaria risk.
Climate variability and changes may influence socio-economic development in Africa by affecting human health through extreme weather events and by bringing about changes in the ecology of infectious diseases. Malaria is a major climate sensitive public health problem in Ethiopia. Unfortunately, there are no practical tools for predicting malaria epidemics based on weather and climate information. Such tools would be useful in making a more efficient use of the limited resources for malaria control.
The project is a collaborative multidisciplinary research project. Researchers from Ethiopia and Norway work together to develop and validate models for predicting malaria transmission and set up an early warning by combining information on climate, water, epidemiological and entomological data. By the end of the project period, EMaPS will try to provide an implementation approach for early malaria warning. The project also aims to strengthen research, and improve interdisciplinary research capacity in Ethiopia and Norway.
The project contains several disciplines (see figure).
The project combined new population-based malaria transmission data with climate and land use variability data to develop early warning to predict malaria epidemics in Ethiopia. Such information is useful for the public and public institutions about the risk of malaria transmission and thus prevents malaria-related deaths.
Overall, eight PhD candidates (six Ethiopians and two Norwegians) take part in the project. The NUFU project funds four of these students, and four are funded by the University of Bergen. They collaborate and share data between the project parts.
We completed the data collection in 2010. During 2011, we mainly focused on data analysis, write-up and publication of the study findings. We expect all PhD candidates to defend their PhD thesis in 2012, and their works are briefly described below.
Abebe Animut is studying malaria mosquitoes in the highlands. He has described the occurrence of Anopheles arabiensis at altitudes as high as 2200m. He has also described the risk of malaria transmission at varying altitudes between 1700 and 2200 m altitude. His study provides good evidence that malaria transmission often occurs in the Ethiopian highlands.
Dereje Tesfahun has evaluated how rainfall and other factors affect the flow of the major rivers in Ethiopia. He has used a model to assess how sensitive the flows of the major river basins are affected by the weather and by possible land use changes. His research shows that Ethiopian rivers are sensitive to precipitation with a 10% change in precipitation giving a 20-30% response in annual stream flow.
Diriba Korecha has studied seasonal weather forecast for Ethiopia. He has re-classified the climatic zones in Ethiopia, worked on models to improve seasonal weather forecasting and validated the result of 10 years of seasonal forecasting in Ethiopia. His research shows that seasonal weather forecasting in Ethiopia is difficult.
Adugna Woyessa has studied the prevalence and risks for malaria using prospective community-based surveys in Butajira in the south central Ethiopian Highlands. His study confirms that malaria is present at altitudes as high as 2200 m, and the malaria prevalence increases towards the lowlands. Malaria occurs throughout the year, but mainly after the main rains. One important finding is that he shows that malaria varies much between villages and within households at all altitudes.
Eskindir Loha studies malaria in the holoendemic Arba Minch area. One of his studies shows that models of climate-malaria link vary from place to place, and one model cannot fit all locations. Malaria modelling may need the inclusion of non-climatic causes. In a follow up study he shows that risk of getting malaria varies much both in time and space within villages. He now works on a paper to describe the influence on rainfall, temperature, socioeconomic factors on the incidence on malaria in these lowlands.
Fekadu Massebo is describing the association between resting behaviour, human blood index and entomological inoculation rates of Anopheles arabiensis in south Ethiopia. The studies include analysis on how mosquito density is associated with malaria cases and how it is influenced by temperature and rainfall. He also assesses insecticide resistance pattern, and if simple house screening will reduce risk of malaria infection.
Torleif Markussen Lunde works on the malaria prediction model. He uses information collected from several disciplines of our project. He has developed a validated malaria prediction model. In the coming months, he will produce malaria distribution maps for Ethiopia, and try to estimate how the new IPPC climate scenarios will affect malaria in the coming years.
Ellen Viste has used weather analysis to describe and analyse from where moisture to Ethiopia comes from. The Indian Ocean, the Congo Basin and the Red Sea are important moisture source regions. The results suggest that most of the air – humid or not – that enters the Ethiopian highlands from the south has travelled through the Indian Ocean, by the African continent, reaching the Ethiopian highlands from the south-west, or through the Turkana channel.
Some conclusions:
The research will reach its research objectives by the end of 2012, and will have produced eight PhDs and over 20 master theses. Based on our experience we conclude the following challenges remain:
Research challenges include:
- Improve seasonal weather forecasting for Ethiopia
- Further develop and field-test malaria prediction in close collaboration with national meteorology and health authorities
- Possibly add new disciplines such as studies on climate – food production and nutrition.
Educational challenges include:
- Strengthen PhD training in advanced epidemiology and mathematical modelling (both in geophysics and in health research)
- Strengthening training in medical entomology (masters level)
These are parts we wish to include in plans for a possible extension of our project.