
The aim of the work is to reduce maternal deaths, reduce deaths among newborns, and increase the number of deliveries at institutions. Our work aims to strengthen the health system by improving work at institutions doing comprehensive emergency obstetrics, and at health centres doing basic emergency obstetric care.
Our work, which consists of training, supervision and equipping and supporting institutions, focus to increase quality of services and better access for women to essential delivery services, and to improve health services for newborn. We thus work with health posts in kebeles, with health centres and hospitals.
We collaborate with the Midwife School in Arba Minch, and currently they are evaluating how good midwives do their work after they graduated from the school. This will give us essential information on how to improve the quality of midwife training, and thus of RMM type of work.
To monitor this work and see if the project meets its societal objectives (reduced death rates), we register births and maternal deaths in four woredas with a population of about 600.000. Our results show that maternal deaths have since 2008 been reduced by 2/3. The number of institutions doing comprehensive emergency care is now about one institution per 250.000 people, a dramatic improvement since 2007 when the figure was one institution per 2.5 million people. The institutional delivery rates have increased substantially, and the use of traditional birth attendants is decreasing. We also see some early signs of decreasing neonatal deaths. In some areas the institutional delivery rates approach 60%. We believe the main reason for these good results is increased access to essential health care.
Even if our results are encouraging, many challenges remain. The birth registration shows that highest maternal deaths rates are among women who live in remote areas, and among women who report illness during pregnancy. One study show that children born to poor women have higher death rates compared with richer families. So, in the coming years will focus on improved quality of care, particularly focusing on improving access, and on managing illness during pregnancy. We will also try to develop tools to identify the poor that are in need of special attention.


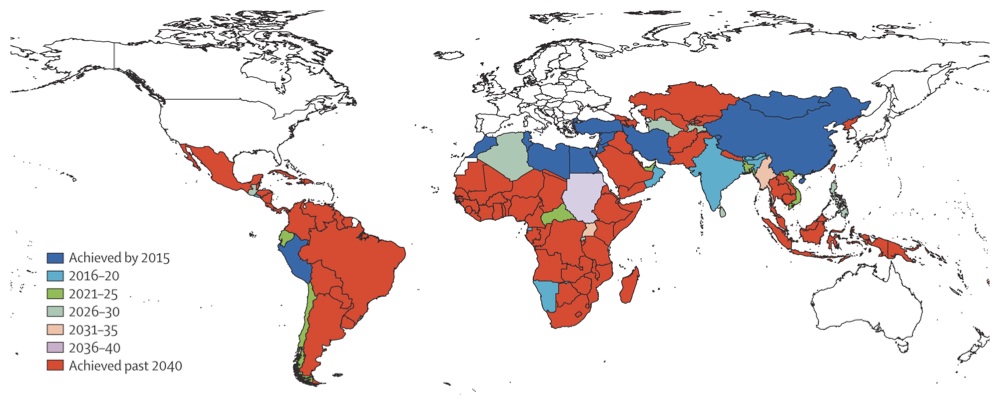 A recent article in The Lancet
A recent article in The Lancet