
Erlend Hem’s Editorial in the Norwegian Medical Journal “Too many journals – too little good research” is thought-provoking, especially the question of whether we publish too much. Fewer and better publications is a good conclusion of his Editorial. But, if we should publish good articles in traditional journals or in electronic “Open Access” (OA) journals is difficult to answer.
OA has improved access to medical journals. Researchers in developing countries can access them free.
Hem suggests that traditional journals have better peer-review than OA journals such as BioMedCentral. I know of examples of articles that have inadequate peer review. However, this applies to both OA and traditional publications. In the research training programme at the University of Bergen, students criticize scientific papers, often from well-known journals such as BMJ and Lancet. And, they often find serious mistakes in the papers.
My question is: Is the editor best suited to choose what is good and important science, and what is essential to publish? And, we know that editors favour scientists they learn to know at conferences and meetings.
Many electronic journals (such as PLoS ONE and BioMedCentral) accepts all submitted articles as long as they meet minimum scientific criteria. Such a policy means that they publish many scientific articles. And such journals have a surprisingly high impact factor, and the best research institutions use them.
Is not it time the Norwegian medical Journal (and other journals) are more “Open Access”? I suggest that all articles that meet the minimum scientific requirements should be published electronically. The Editor can then choose articles they wish to publish in the printed paper version.
(This is a translation of the Norwegian text on the Journal’s blog)

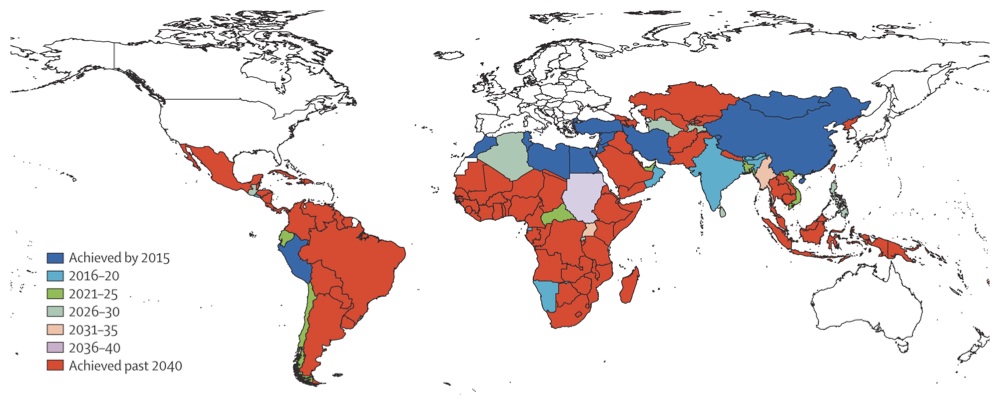 A recent article in The Lancet
A recent article in The Lancet")
{kind=link}